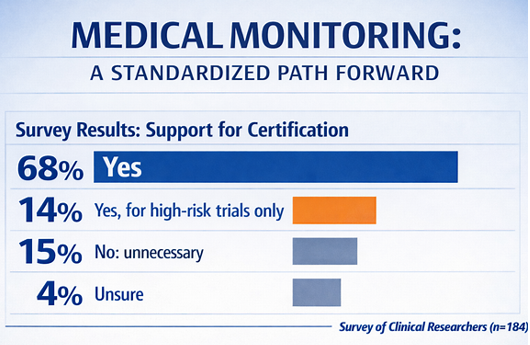
LinkedIn poll results suggest interest in a “formal certification process”
Authors: Gerald L. Klein, MD[1]; Roger Morgan, MD[1]; Melissa Palmer, MD[2]; Freddy Byrth, BS[1]; Patrick Loebs, MSW, MPH[1]; Stephen Haworth, MB[1]; Emila Jones, MD[3]; Katie Louise Dawson, MD[1]
Affiliations: MedSurgPI[1]; Liver Consulting, LLC[2]; EJ Med Insights[3]
Medical monitoring operates within one of the most consequential intersections in clinical research: participant safety, protocol integrity, regulatory compliance, clinical judgment, and real-time operational decision-making. Yet despite its importance, the role remains inconsistently defined across sponsors, clinical research Organizations (CROs), therapeutic areas, and study phases and types.
For the purposes of this discussion, medical monitoring is defined as medically qualified oversight that supports participant safety, protocol interpretation, participant eligibility, medical-data review, safety surveillance, escalation of emerging risks, and clinical decision support to sponsors, CROs, investigators, and safety governance bodies.
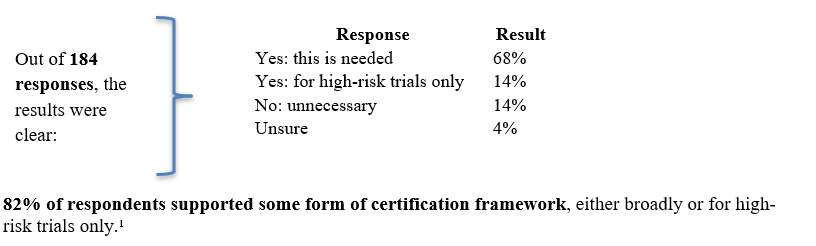
We recently surveyed the clinical research community in a LinkedIn poll through the following question with one of four possible responses. To ensure the poll reached the appropriate audience, we distributed it specifically within LinkedIn groups composed of clinical research professionals. Although this represents a relatively small sample of the broader clinical trial community, we believe the responses offer a meaningful anecdotal reflection of prevailing community perspectives.
That is a meaningful signal. While the sample size is limited, the results suggest meaningful professional recognition of a growing gap in standardization. The broader conversation is shifting from whether medical monitoring matters to how it should be defined, supported, and documented. It is now a question of whether the industry should define a consistent standard, who performs medical monitoring, what competencies are required, and how readiness is demonstrated.
Why does this question matter now?
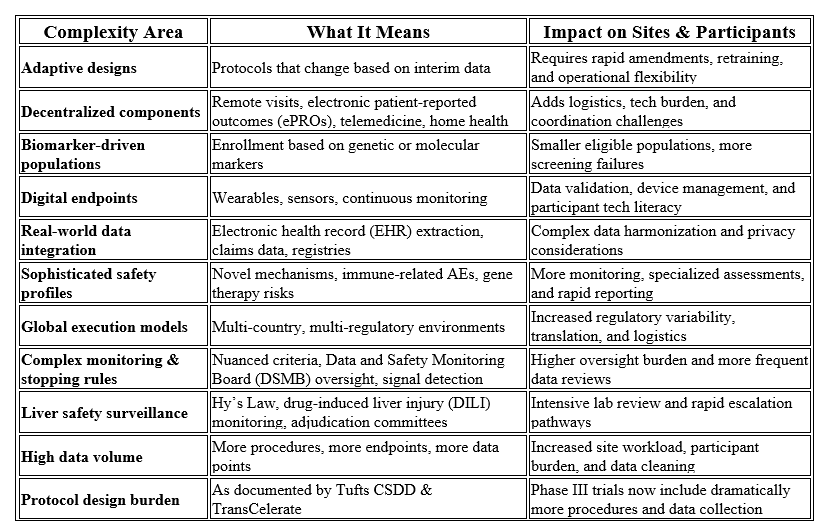
Clinical trials are becoming increasingly complex across scientific, operational, and regulatory dimensions. Protocols now frequently incorporate adaptive designs, decentralized elements, biomarker‑defined populations, digital endpoints, real‑world data, sophisticated safety requirements, global execution models, and intricate monitoring or stopping criteria. These factors, combined with substantially higher data volumes, create significant burden for both participants and research sites. Recent analyses from the Tufts Center for the Study of Drug Development (CSDD) and TransCelerate BioPharma both confirm that Phase III pivotal trials now involve far more procedures and data points than in previous decades, underscoring the accelerating complexity of modern clinical research.²
Table 1 summarizes these drivers of complexity and their operational impact on sites and participants.
At the same time, global regulatory expectations are moving toward risk-based quality management, proportionality, quality by design, and clearer accountability. The new International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) E6(R3) Good Clinical Practice (GCP) guidance emphasizes flexible, risk-based approaches, quality by design, participant protection, reliability of trial results, and clarified sponsor and investigator responsibilities.³ The FDA’s risk-based monitoring guidance similarly focuses sponsor oversight on the most important aspects of study conduct and reporting to enhance human subject protection and data quality.⁴
In other words, the industry is being asked to become more agile and adopt more risk-based operational strategies, while trials are becoming more medically, operationally, and technologically complex. Medical monitoring expertise is central to that transition to more complex studies and greater safety oversight.
The standardization gap
Current regulations and guidance establish sponsor accountability for appropriate monitoring, safety review, and use of qualified personnel. For example, FDA regulations state that sponsors are responsible for ensuring proper monitoring of investigations, and that sponsors must select monitors qualified by training and experience.⁵ The National Institutes of Health (NIH) policy also recognizes the medical monitor as a possible data and safety monitoring entity and states that monitoring plans should be commensurate with the level of risk, nature and complexity of the research, and population under study.⁶
However, regulators generally do not define a standardized role-specific set of competencies for the modern medical monitor, and current expectations do not translate into a single, industry-wide, regulator-recognized standard. In practice, the role may vary substantially from one organization to another. In some studies, the medical monitor is deeply involved in protocol development, eligibility review, safety surveillance, adverse event assessment, protocol deviation review, medical data review, site escalation, investigator support, and DSMB or safety committee interactions. In others, the role is narrower, reactive, or insufficiently documented.
That variability creates risk. Not necessarily because some medical monitors lack expertise, but because the industry lacks a consistent way to define, verify, and maintain the competencies required for the role. And sometimes medical monitors do lack the necessary expertise.
What the poll tells us
The poll results suggest that the industry supports medical monitor certification. A practical model could include a common baseline certificate, an advanced certificate for high-risk or complex trials, and optional therapeutic-area or modality modules.
The goal should not be to create another administrative hurdle or to imply that certification can replace clinical experience. Poorly designed certification programs would add cost without improving results. The value of a framework would depend on whether it is practical, case-based, risk-proportionate, and clearly tied to decisions medical monitors make during trial conduct.
What a practical framework could look like
A practical medical monitoring certification framework should be demonstrated around competency, judgment, and risk, not paperwork. A useful model could include three levels:
1. Foundational Medical Monitoring Certification
This would apply to physicians or qualified health-care professionals supporting clinical trials. Core competencies would include GCP, regulatory responsibilities, participant protection, informed consent process, safety surveillance, adverse event assessment, protocol interpretation, medical data review, documentation standards, and clearly defined escalation pathways.
2. Advanced Certification for High-Risk or Complex Trials
This level would be intended for medical monitors supporting studies with elevated medical, operational, or regulatory complexity, including first-in-human trials, complex oncology programs, rare disease studies, gene and cell therapy development, high-risk device investigations, adaptive or platform trial designs, and research involving vulnerable populations. Additional competencies could include dose-escalation governance, monitoring, pausing, and stopping criteria, emerging safety signal management, benefit-risk assessment, DSMB/Data Monitoring Committee (DMC) interface, blinded vs. unblinded safety management processes, and crisis escalation procedures.
3. Therapeutic Area or Modality Modules
Optional specialization modules could further strengthen this framework by addressing therapeutic areas and operational domains where medical monitoring demands distinct expertise such as oncology, immunology, infectious disease, hepatology, neurology/CNS, cardiovascular, endocrinology, dermatology, gastroenterology, rare disease, pediatrics, women’s health, medical devices, digital endpoints, advanced biologics, gene and cell therapies, real world evidence integration, decentralized trials, or advanced therapies. This would preserve flexibility while recognizing that medical monitoring expertise is not interchangeable across all contexts.
To avoid becoming a “check-the-box” exercise, certification should include case-based assessment, continuing education, conflict-of-interest principles, documentation expectations, and periodic renewal. It should also clarify the medical monitor’s relationship matrix regarding trial conduct with the sponsor, investigator, CRO, safety management team, pharmacovigilance function, and independent DMC/DSMB when applicable. FDA’s DMC guidance underscores the importance of determining when independent committees are useful and how their operation should be structured; a medical monitoring framework should complement, not duplicate, that oversight.⁷
To bring this idea to life, Table 2 below shows how certification can stay meaningful, grounded in real‑world case work and clear professional boundaries. It highlights the essential competencies and the relationships that define effective medical monitoring oversight.
Table 2: Medical Monitoring Certification Framework
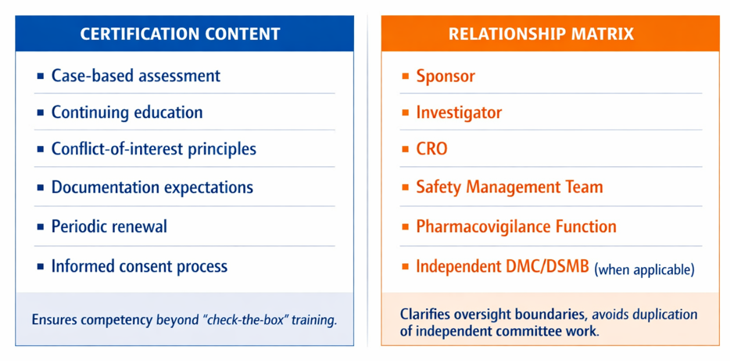
The right framework would not replace sponsor accountability, therapeutic expertise, clinical judgment, or trial-specific training. It would create a common baseline for what “qualified” means in practice and provide a more transparent way to demonstrate readiness for a role that directly affects participant safety and trial integrity.
A practical and achievable initial step would not need to be a regulator-mandated credential. Instead, the industry could begin with a voluntary consensus-based competency framework developed collaboratively by key stakeholders including sponsors, CROs, academic clinical trialists, professional societies, experienced medical monitors, patient representatives, and regulatory bodies. Such an approach would allow for scalable standardization while preserving flexibility and stakeholder alignment. An initial pilot program could reasonably focus on high-risk interventional trials, where oversight demands are the greatest, competency gaps may carry the highest consequences, and the potential value of standardized medical monitoring qualifications is most immediately evident.
A call to action
The poll’s message is clear: the clinical research community sees a gap and is ready to discuss solutions.
Moving forward, progress will likely require a collaborative, multi-stakeholder approach. Sponsors, CROs, investigators, regulators, professional societies, academic medical centers, patient representatives, and experienced medical monitors should work together to define a practical competency framework. An initial pilot approach focused on high-risk trials, where the need is most obvious and the value proposition is strongest.
Medical monitoring has evolved well beyond a purely supportive role and now functions as a strategic safeguard for participant safety, protocol integrity, and risk management. As clinical trials continue to increase in complexity, reliance on inconsistent interpretations of this role may no longer be sufficient.
While a formal, risk-based certification framework would not eliminate sponsor accountability, clinical judgment, or trial-specific training, it could represent an important step toward consistency, transparency, and trust.
The question is no longer whether medical monitoring is essential; the question is whether we are ready to define the standard it deserves.
Disclaimer: This issue references an informal poll conducted on LinkedIn. LinkedIn did not sponsor, endorse, or participate in the poll. Content is for general informational purposes only.