From East Carolina School of Dentistry Research Division and MedSurgPI
Authors: Gerald L. Klein, MD1; Alexandre R. Vieira, DDS, MS, PhD2; Stephen Haworth, MB, BS1; Freddy Byrth, BS1; Roger Morgan, MD1; Rob Walsh, MD1; Larry Florin, MBA3
Affiliations: MedSurgPI, LLC1; East Carolina University School of Dental Medicine2; LBF Biopharma Consulting3
Why Primary Care Should Ask, Look, Treat, and Refer
Practical pointer: A one-minute oral-health questionnaire paired with a quick visual check of the mouth helps primary care teams identify pain, infection, cancer warning signs, dry mouth, caries risk, periodontal risk, and lack of dental access. The goal is not to make primary care a dental office; it is to close a common gap by counseling, applying evidence-supported preventive care when appropriate, treating urgent medical consequences, and arranging timely dental referrals.
The mouth is part of the body, but it is often left outside routine medical care. That separation matters. CDC surveillance data show that nearly 21% of U.S. adults aged 20-64 had untreated decay in permanent teeth, with higher burden among people living in poverty, some racial and ethnic groups, (for example, American Indian/Alaska Native, African American and other historically marginalized populations), people with lower educational attainment, and current smokers.[1] Untreated oral disease can produce pain, infection, tooth loss, difficulty eating and speaking, missed school and work, and avoidable emergency visits.[2]
Primary care is uniquely positioned to help. Patients with diabetes, pregnancy, xerostomia, tobacco or alcohol use, immunosuppression, chronic disease, medication burden, or poor access to dental care are already in our exam rooms. A simple oral-health workflow can be framed as Ask, Look, Decide, Act, and Document/Follow Up - a model described for primary care integration by the National Academy of Medicine and the Oral Health Delivery Framework.[3]
This is a practical clinical screen, not a substitute dental diagnosis. The United States Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against routine primary-care screening or preventive interventions for asymptomatic adults and for children/adolescents aged 5-17. That insufficient “evidence statement” should not be read as a recommendation to ignore the mouth; it means the evidence is incomplete and clinicians should use judgment. However, Rural America has a greater incidence of oral problems and recommends a greater need for this intervention.[4] The stronger primary care role is to identify symptoms and risk, deliver brief prevention, and connect patients to dental care. For children younger than 5 years, the USPSTF specifically recommends fluoride varnish after primary tooth eruption and oral fluoride supplementation from age 6 months when the water supply is fluoride deficient.[5],[6]

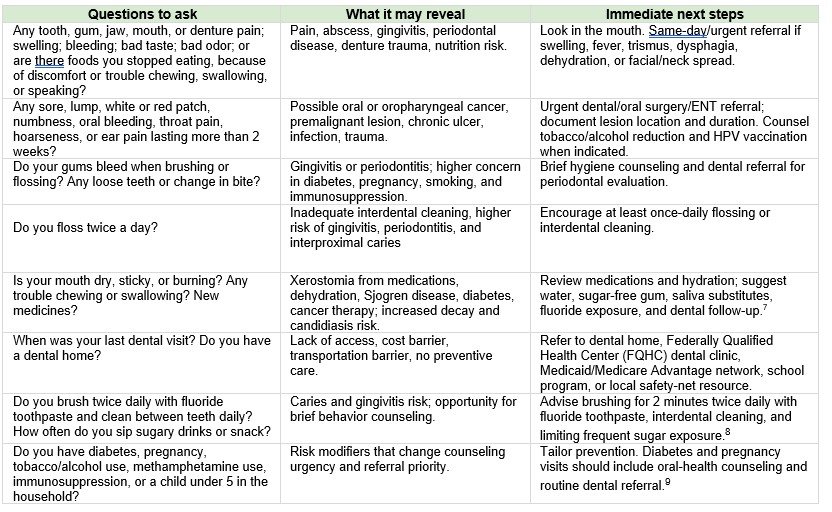
A short questionnaire for primary care
Use these questions at annual visits, well-child visits, diabetes visits, pregnancy visits, medication reviews, transitions of care, and visits for pain, fever, swelling, weight loss, or nutrition problems. A positive answer should prompt a brief mouth exam and a clear follow-up plan.
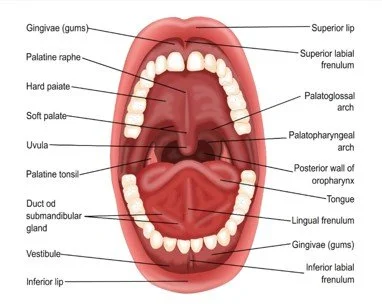
The brief mouth look
Use gloves, a light, and a tongue blade. Inspect the lips, buccal mucosa, tongue and floor of mouth, palate, gingiva, teeth, dentures, and visible oropharynx. Note saliva quality, odor, plaque, visible decay, broken teeth, gingival swelling, ulcers, white patches that scrape or do not scrape, red patches, masses, facial swelling, trismus, and ability to swallow. If clinic policy allows photos, obtain consent and include images in the referral. CDC lists oral-cancer symptoms such as nonhealing sores, swelling or unusual bleeding, difficulty breathing/speaking/ chewing/swallowing, and persistent mouth or throat pain; tobacco and alcohol are common risk factors, and HPV is linked to some oropharyngeal cancers.[1]
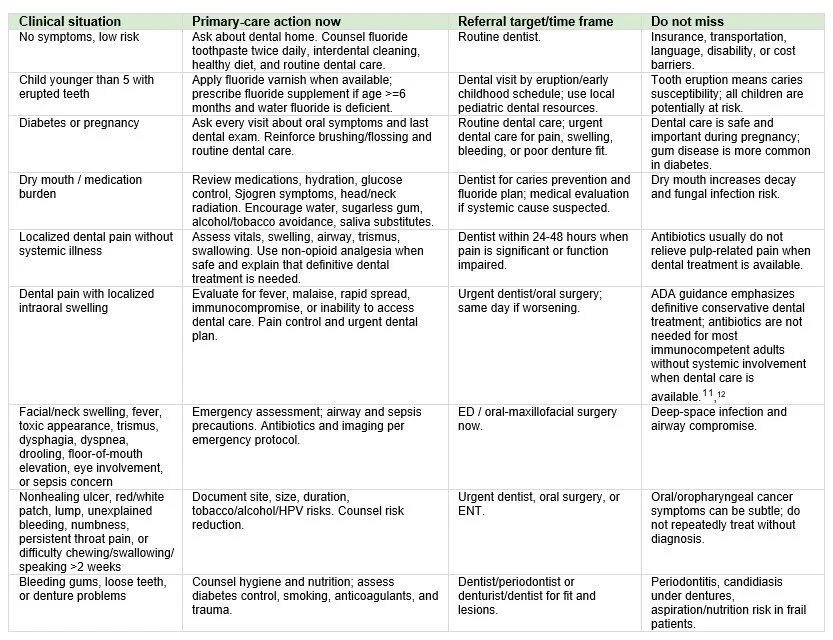
Preventive and therapeutic actions
Most oral diseases require definitive dental care. Primary care can still reduce harm by triaging urgency, treating medical complications, and making referral specific rather than vague.
Make referral closed-loop, not aspirational
A strong oral-health plan is specific: name the concern, urgency, destination, and follow-up. For example: “localized dental swelling without fever, urgent dental appointment within 48 hours; call if fever, worsening swelling, difficulty swallowing, or breathing symptoms.” Build a dental referral list that includes practices accepting Medicaid, Federally Qualified Health Center (FQHC) dental sites, pediatric dentists, oral surgeons, ENT clinics, pregnancy-capable dental practices, and after-hours emergency pathways. Document the questionnaire response, mouth findings, treatment/counseling, referral, and how the team will confirm completion. Because oral disease contributes to significant productivity and school losses nationally, prevention and care navigation should be considered essential elements of primary care, not add-ons.[1]
Oral cancer: An estimated 60,500 new cases will be diagnosed in 2026.[2] They are usually diagnosed late; primary care examination may help to modify this current situation.
Bottom line: Primary care should evaluate the mouth because oral problems are common, visible, consequential, and often missed. A short questionnaire, a quick look, brief prevention, targeted therapy, and closed-loop referral can prevent avoidable suffering while respecting the essential role of dental professionals.
[1] Centers for Disease Control and Prevention. Oral Health Facts. May 15, 2024. https://www.cdc.gov/oral-health/data-research/facts-stats/index.html
[2] CDC, 2024 Oral Health Surveillance Report: Selected Findings; USPSTF, Oral Health in Adults: Screening and Preventive Interventions, 2023.
[3] National Academy of Medicine, Integration of Oral Health and Primary Care: Communication, Coordination and Referral; Oral Health Delivery Framework: Ask, Look, Decide, Act, Document & Follow-Up.
[4] U.S. Preventive Services Task Force. USPSTF Procedure Manual. 2021. Accessed May 13, 2026. https://www.uspreventiveservicestaskforce.org
[5] USPSTF, Prevention of Dental Caries in Children Younger Than 5 Years: Screening and Interventions, 2021.
[6] USPSTF, Oral Health in Adults: Screening and Preventive Interventions, 2023; USPSTF, Oral Health in Children and Adolescents Aged 5 to 17 Years, 2023.
[7] National Institute of Dental and Craniofacial Research, Dry Mouth.
[8] American Dental Association, Home Oral Care, updated 2024; American Dental Association, Topical Fluoride Clinical Practice Guideline, 2013.
[9] CDC, Promoting Oral Health for People With Diabetes, 2024; CDC, Dental Care Is Safe and Important During Pregnancy, 2024.
[10] CDC, About Oral Cancer, 2024.
[11] American Dental Association, Antibiotics for Dental Pain and Swelling Guideline, 2019; endorsed by the American College of Emergency Physicians.
[12] American Dental Association. Antibiotics for Dental Pain and Swelling Guideline. 2019. https://www.ada.org/resources/research/science/evidence-based-dental-research/antibiotics-for-dental-pain-and-swelling
[13] CDC, Oral Health Facts, 2024.
[14] American Cancer Society. Key Statistics for Oral Cavity and Oropharyngeal Cancers. Updated March 23, 2026.