MedSurgPI's, Dr. Peter Johnson will chair this conference which will take place August 5-10, 2018 in Andover, NH. Click here to link directly to the conference site.
Your Custom Text Here
MedSurgPI's, Dr. Peter Johnson will chair this conference which will take place August 5-10, 2018 in Andover, NH. Click here to link directly to the conference site.

MedSurgPI is the preeminent Physician Functional Service Provider. We provide medical strategy, medical monitoring, medical affairs, and medical writing from our experienced physician team of seasoned executives. Our goal is to provide this outsourced service to increase efficiencies and decrease cost for drug, device, diagnostic, and nutritional development services.
MedSurgPI doctors are flexible and can provide short term assistance or long term collaboration.
Whether you want a medical strategy, clinical trial guidance, medical monitor or an interim Chief Medical Officer, contact MedSurgPI, LLC at: info@medsurgpi.com.
James D. Hundley, M.D., Physician Associate with MedSurgPI, LLC has co-authored a book My Hip Hurts!: Causes and Treatment of Hip Pain in Seniors. Authors Dr. Hundley and Richard J. Nasca, M.D. are two orthopaedic surgeons with over 100 combined years of training and experience. This is an exciting book as Drs. Hundley and Nasca describe conditions of the hip suffered by older people, what can be done for them, and what they would recommend. Simple drawings and x-rays are used for illustration along with a glossary to help understand medical terms.
This book is available through Amazon at the following link: My Hip Hurts!: Causes and Treatment of Hip Pain in Seniors
Aparna Shekar1,2, Gerald L. Klein, MD3, and Peter C. Johnson, MD3
1Ph.D. Candidate, Vanderbilt University, Nashville TN, 2Intern, MedSurgPI, LLC., Raleigh NC, 3Principal, MedSurgPI, LLC., Raleigh NC

Clinical trials are scientific experiments designed to test new medications, devices or other therapeutic interventions, or to further gain insight on those treatments for use in human medicine. They aim to produce insight into the safety and efficacy of medical interventions and strive to produce improvements in medical care. Clinical trials have evolved substantially since James Lind’s Scurvy trial in the 1700s1, to become more structured and supervised, and to generate more rigorous, reproducible results. But along with being thorough came a new set of challenges - clinical trials today face a gamut of scientific, ethical, regulatory and financial roadblocks. Biopharmaceutical development is a global business today. Companies are routinely conducting clinical trials in foreign nations with the intent that the data will also to be used to support US claims2,3. In 2008, 80% of all marketing applications submitted to the FDA contained data from foreign clinical trials (https://oig.hhs.gov/oei/reports/oei-01-08-00510.pdf). There are several reasons for this trend, including but not limited to lower costs of conducting trials abroad. In 2013, the Tufts Center for the Study of Drug Development estimated that the total costs for developing, seeking approval and marketing a new chemical entity costs $2.6 billion on average, creating an impetus for decreasing the costs of clinical trials. Countries that have grown to be popular choices for conducting clinical trials include those in Latin America, Asia, Europe and Africa where lower operating costs occur. Some of these lower costs include human resources, clinical procedure costs, site monitoring costs, regulatory, and compensation in case of injuries/deaths that may occur4. Other significant benefits of foreign clinical trials include the ability to enable globalized medical product discovery and development, expand diversity of the test subject pool, shorten drug development timelines and less litigious and, importantly, to test patients that are naive to treatments not found in third world countries. Due to these advantages, the number of foreign clinical trials conducted to meet US FDA regulations has more than doubled over the past decade.
However, there are major risks involved in conducting clinical trials outside the United States. Companies need to consider and prepare in advance to understand country-specific insurance requirements, legal restrictions and regulations regarding conducting clinical trials with human subjects. They also need to determine if the trial design conforms to FDA standards so that trial data can be accepted by the FDA for review. In the absence of prior careful consideration, sponsors may inadvertently violate local insurance laws, expose themselves to excessive liability, or even unknowingly purchase insurance coverage that is well beyond the requirements of a particular country. It is particularly important for sponsors to thoroughly understand and follow FDA guidelines for conducting clinical trials in a foreign country. Under Section 1123 of the Food and Drug Administration Safety and Innovation Act (FDASIA) of 2012, data from foreign clinical trials should be accepted by the FDA, provided such studies comply with U.S. federal standards on Good Clinical Practices (GCPs). As of 2016, the FDA has issued guidelines stating that it may accept clinical trials conducted outside the US under the classification of an Investigational New Drug (IND) and comports with all FDA regulations as if the trial were being conducted within the United States. Additionally, it may consider a trial not conducted under the classification of IND, so long as the study conforms to whichever of the following rules provides greater protection of the test subjects: (i) the ethical principles contained in the 1983 version of the Declaration of Helinski or (ii) human rights regulations in the foreign country in which the trial is conducted. The new Questions and Answers (Q&A) Guidance from the FDA issued on February 21, 2018 provides further clarification on how to conduct these trials. The International Conference on Harmonization (ICH) and World Health Organization Good Clinical Practice (GCP) standards provide a unified measurement for the USA, European Union, Japan, Australia, Canada, the Nordic countries and several others. A complete list of countries that have adopted this guideline is available online at www.ich.org. Additionally, research groups have also developed methods that can predict country-specific financial requirements, outcomes of trials and risks involved in foreign locations that are developing countries, that may help sponsors in identifying an appropriate country in which to conduct their trial5,6. This new Q&A guidance document emphasizes the importance of a description of how investigators were trained to comply with GCP and how the study was monitored so that the investigations were done in accordance with the protocol (Section 812.28(b)(12)).
Ultimately, it is important to maintain scientific integrity and patient safety, which leads to better trial outcomes. Several resources are available that can help companies understand the strict guidelines that they are required to follow to manage potential risks. Companies can seek aid from experts on ICF and GCP guidelines, foreign insurance policies, medical insurance policies, informed consent requirements and FDA liaisons. Our experts from MedSurgPI, LLC. can aid pharmaceutical and medical device companies in making informed decisions and adopting appropriate steps before they embark on conducting clinical trials in foreign countries. MedSurgPI, LLC. by providing experienced product development expert services to its clients is well positioned to bridge the business and medical understanding that such risk management requires.
References:
1 Lind and scurvy - 1747 to 1795.
2 Capeding, M. R. et al. Clinical efficacy and safety of a novel tetravalent dengue vaccine in healthy children in Asia: a phase 3, randomised, observer-masked, placebo-controlled trial. The Lancet 384, 1358-1365, doi:10.1016/s0140-6736(14)61060-6 (2014).
3 Ezeome, E. R. & Simon, C. Ethical problems in conducting research in acute epidemics: the Pfizer meningitis study in Nigeria as an illustration. Dev World Bioeth 10, 1-10, doi:10.1111/j.1471-8847.2008.00239.x (2010).
4 Dezfuli, M. Outsourcing Clinical Trials Outside of the US. Pharmaceutical Regulatory Affairs: Open Access 06, doi:10.4172/2167-7689.1000194 (2017).
5 Lorenzo, C., Garrafa, V., Solbakk, J. H. & Vidal, S. Hidden risks associated with clinical trials in developing countries. J Med Ethics 36, 111-115, doi:10.1136/jme.2009.031708 (2010).
6 Hidden risks associated with clinical trials in developing countries.
FEBRUARY 5, 2018 (PITTSBURGH, PA) – Microbac Laboratories, Inc. today announces a new strategic partnership to offer clients the R&D consulting services of MedSurgPI - a team of commercially experienced pharmaceutical and medical device consultants. Click to read full story.


We have been amazed at the complexity of the journey of clinical supplies to investigator sites is and delays can be extremely costly for sponsors. In fact, supply chain logistics can account for up to 25% of total annual pharmaceutical R&D costs. With stakes this high, it’s important to understand the strengths and weaknesses of tools uses to plan such critical projects.
Spreadsheet Models
The most common tool used for planning and managing Clinical Supply Chains are spreadsheet models. While this approach has some attractive qualities (simplicity, familiarity, and ease of sharing results) they suffer from several drawbacks.
For basic or static analysis, spreadsheets are often the right tool. However, supply chains are not static. They have parameters, resource constraints, queues, and demand curves that will change over time. This is where spreadsheet models show their limitations in capturing real-world situations. Although they will provide an answer, if you only use averages as your inputs, you will always get the average result, and not the range of real-world possibilities.
Simulation
Due to the drawbacks of spreadsheet models, approximately 10% of pharma companies have tried to solve these shortcomings by utilizing more sophisticated, dynamic tools like simulation. However, while simulation solves many of the shortcomings of spreadsheet models, they also introduce new problems; namely complexity and lack of transparency. Developing realistic simulations of supply chains is not an easy task because the software is often proprietary and the learning curve for programming them can be extremely high unless you are a data scientist or software developer.
Due to these barriers, the management of clinical trial supply chains and approaches to minimize costs has received little attention in formal research [Chen, Mockus, Orcun, & Reklaitis, 2012]. Much of the research that has been done does not consider the inherent randomness found in real-world clinical supply chain systems. This makes much of the research less applicable to pharma companies because uncertainty and variability is inherent to patient enrollment, shipment lead times, and process delays [Chen et al., 2012].
Alternatives
Given the challenges with both spreadsheet models and simulation, what are clinical trial supply chain decision makers to do? There are two possible solutions:
1) Develop highly intricate and complex simulation models using Discrete Event Simulation (DES) software like ExtendSim (https://goo.gl/VFSHak) or Python SimPy in hopes of capturing all the aspects of a complex supply chain; or
2) Simply eliminate the need and cost of the supply chain by providing subjects with a clinical study pharmacy card.
Some pharma companies take the first route and try to model complex clinical trial supply chains in hopes of maximizing efficiency and expediting clinical trials. Although not the easiest route, companies that wish to pursue this path would benefit from developing an understanding of dynamic programming and simulation optimization strategies. A good starting point would be a paper by Jung, Blau, Pekny, Reklaitis, and Eversdyk (2004), covering a simulation optimization approach to solve a generalized supply chain problem under demand uncertainty.
Using the RxStudyCard Instead of trying to build a large-scale simulation and then run hundreds of scenarios in hopes of identifying efficiencies, decision makers can simply eliminate much of it using a clinical study pharmacy card which leverages a network of over 60,000 retail pharmacies to deliver medicine and supplies to subjects participating in clinical studies. This type of program provides a safe and efficient method of dispensing unblinded medicines and supplies to study subjects that saves administrative effort, wasted supply overage, and time as well as reduces the amount of capital expense required by 30 to 60%, depending on the size of the study.
Chen, Ye, Linas Mockus, Seza Orcun, and Gintaras V. Reklaitis. “Simulation-Optimization Approach to Clinical Trial Supply Chain Management with Demand Scenario Forecast.” Computers & Chemical Engineering 40, no. Supplement C (May 11, 2012): 82–96. https://doi.org/10.1016/j.compchemeng.2012.01.007.
Jung, June Young, Gary Blau, Joseph F. Pekny, Gintaras V. Reklaitis, and David Eversdyk. “A Simulation Based Optimization Approach to Supply Chain Management under Demand Uncertainty.” Computers & Chemical Engineering, Special Issue for Professor Arthur W. Westerberg, 28, no. 10 (September 15, 2004): 2087–2106. https://doi.org/10.1016/j.compchemeng.2004.06.006.
This service is a proprietary process to assist start-ups and established Life Science companies launch their drug, diagnostic and medical device products successfully from concept through launch and post-market surveillance. It encompasses proof-of-concept studies, clinical trial assistance, market research, product development, health economics and outcomes research services, a successful launch, data analytics and pharmacovigilance.
MD to Entrepreneur: From bedside to boardroom
Shabnam Vaezzadeh, MD, MPA, Gerald L. Klein, MD, Peter C. Johnson, MD,
Valerie Riddle, MD, Robert L. Wolfert, PhD

Gerald L. Klein, MD (MedSurgPI), Celine Clive (Polaris Compliance Consultants),
Peter C. Johnson, MD (MedSurgPI), Laurie Meehan (Polaris Compliance Consultants),
Roger Morgan, MD (MedSurgPI) and Valerie Riddle, MD

David Lengacher (Rx Solutions), Gerald L. Klein, MD (MedSurgPI LLC), Peter C. Johnson, MD (MedSurgPI, LLC), Roger E. Morgan MD (MedSurgPI, LLC), Valerie Riddle MD and Brent Walter (Rx Solutions)

Peter C. Johnson, MD*, June S. Almenoff, MD**, PhD and Gerald L. Klein, MD*
MedSurgPI, LLC*, Raleigh, NC and ** Independent Drug Development Consultant, Durham, NC*

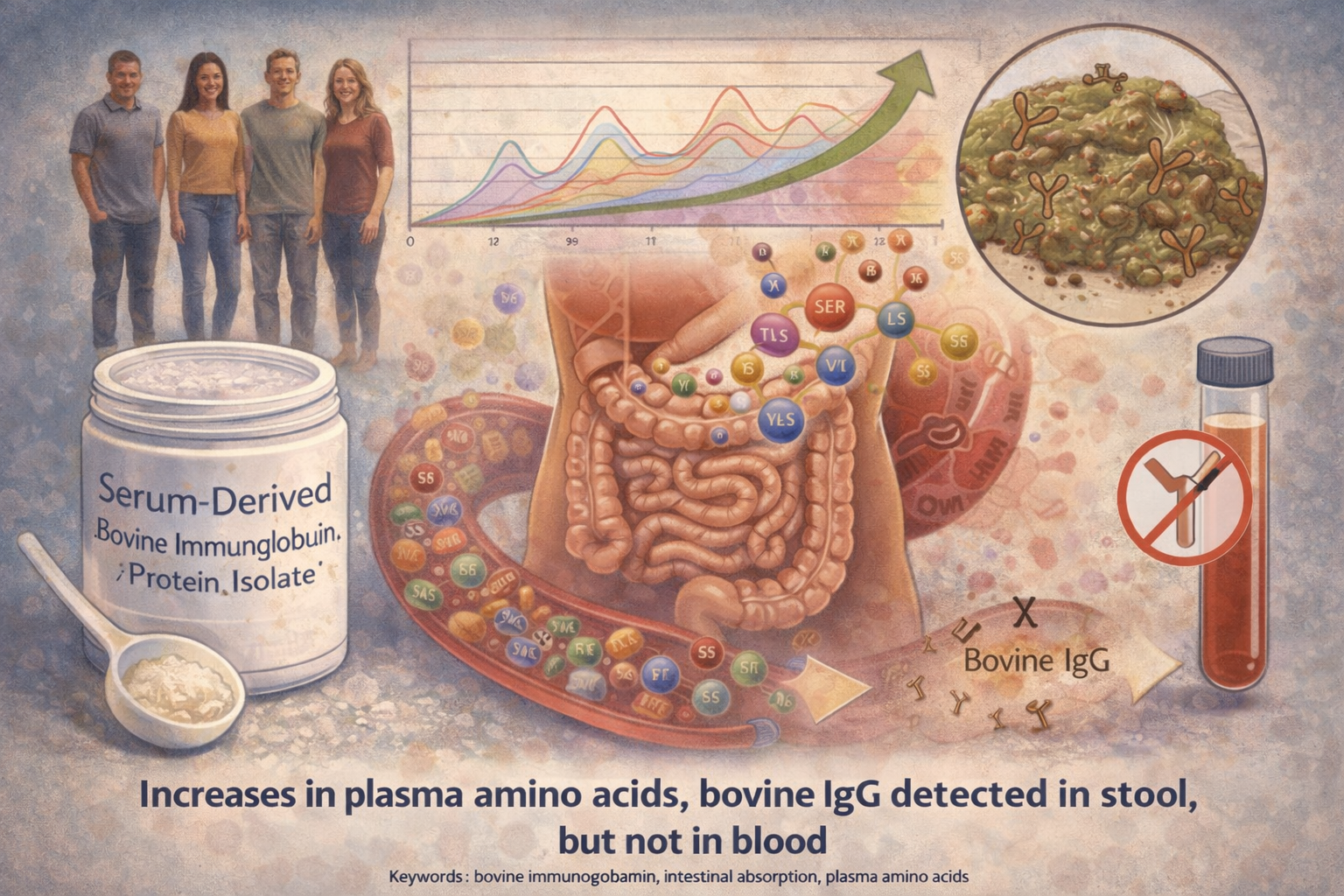
Authors: Audrey L Shaw, PhD; David W Mathews, John E Hinkle, PhD; Bryon W Petschow, PhD; Eric M Weaver, PhD; Christopher J Detzel, PhD; Gerald L Klein, MD; Timothy P Bradshaw, PhD
Purpose: Previous studies have shown that oral administration of bovine immunoglobulin protein preparations is safe and provides nutritional and intestinal health benefits. The purpose of this study was to evaluate the plasma amino acid response following a single dose of serum-derived bovine immunoglobulin/protein isolate (SBI) and whether bovine immunoglobulin G (IgG) is present in stool or in blood following multiple doses of SBI in healthy volunteers. Methods: A total of 42 healthy adults were administered a single dose of placebo or SBI at one of three doses (5 g, 10 g, or 20 g) in blinded fashion and then continued on SBI (2.5 g, 5 g, or 10 g) twice daily (BID) for an additional 2 weeks. Serial blood samples were collected for amino acid analysis following a single dose of placebo or SBI. Stool and blood samples were collected to assess bovine IgG levels. Results: The area under the curve from time 0 minute to 180 minutes for essential and total amino acids as well as tryptophan increased following ingestion of 5 g, 10 g, or 20 g of SBI, with a significant difference between placebo and all doses of SBI (p<0.05) for essential amino acids and tryptophan but only the 10 g and 20 g doses for total amino acids. Bovine IgG was detected in the stool following multiple doses of SBI. No quantifiable levels of bovine IgG were determined in plasma samples 90 minutes following administration of a single dose or multiple doses of SBI. Conclusion: Oral administration of SBI leads to increases in plasma essential amino acids during transit through the gastrointestinal tract and is safe at levels as high as 20 g/day





